

Authored by Lawrence Wilson via The Epoch Times (emphasis ours),
Medicaid is a broadly popular program that provides medical coverage to low-income Americans through a combination of state and federal funding. More than 60 percent of Americans either know someone who has benefited from Medicaid or have been enrolled themselves, according to health policy think tank FFF. So any talk of altering the program usually meets strong opposition.

Yet few seem to know how the system works, what it costs, or the level of unnecessary spending hidden within its $880 billion annual budget.
One example is a little-known quirk in the Medicaid system that allows states to artificially inflate their Medicaid costs to recoup more federal dollars. The arrangement allows some states to pocket a share of the money paid to them for providing treatment to Medicaid patients.
Here’s how it works.

The Loophole
When a Medicaid patient receives a treatment or service, the state pays the doctor, hospital, nursing home, or other provider. The federal government reimburses each state for a portion of its Medicaid expenses. The reimbursement ranges from 50 to 76.9 percent depending on the income level in the state and other factors.
Although, for people who enrolled through the Medicaid expansion under the Affordable Care Act, the reimbursement rate is 90 percent.
So if a state had a 60 percent reimbursement rate and spent $10 billion on Medicaid services, the federal government would reimburse the state $6 billion.
That’s how the system was designed to work back in 1965, generally speaking.
By the mid-1980s, some states had found a way to increase payments to providers and their own Medicaid costs at the expense of the federal government.
First, medical providers would either voluntarily donate money to a state or agree to pay a tax. The states would then return the amount of the donation or tax, and possibly even more, through increased reimbursement. Finally, the states would bill the federal government for the increased cost.
In some cases, the providers initiated these arrangements, according to the Congressional Research Service (CRS).
For example, a hospital might agree to pay the state $10 million in taxes. The state might then increase Medicaid payments to that hospital by $20 million. If the state’s reimbursement rate was 60 percent, it would receive $12 million in federal Medicaid funding.
Together with the tax income, the state would receive $22 million and pay $20 million, netting $2 million for additional Medicaid costs or other purposes.
The arrangement benefited providers by increasing their reimbursement, and the states benefited by reducing their costs or even gaining revenue. The federal government bore the cost of those increases.
Congress debated the issue in 1991.
Lawmakers who favored keeping the arrangement in some form argued that it had become a vital part of state Medicaid funding.
Rep. Raymond McGrath (R-N.Y.) said at the time that doing away with the system would cost his state $500 million in federal matching funds. He predicted “chaos” in the Medicaid system if provider taxes were abolished.
The administration of President George H.W. Bush strongly opposed the taxes in a position statement, saying, “State donation and provider-specific tax programs, if unchecked, will undermine a basic premise of the Medicaid program—that States have a stake in the costs of the program.”
In the end, Congress chose to impose limits on provider taxes and donations.
First, provider donations to the state are strictly limited to prevent abuse. Second, state taxes must meet certain conditions or the state will lose federal funding.
Taxes must apply to all providers in a certain class, such as nursing homes, not just those who serve Medicaid patients. Also states can’t provide any direct or implied guarantee that they will reimburse providers for the amount of the tax. The limit on provider taxes is 6 percent.
Here’s how the provider tax works today.

Increasing Tax, Dependence
In 2004, 35 states had taxes on medical care providers. Now every state but Alaska taxes some providers, as does the District of Columbia.
And states depend more on tax revenue to fund Medicaid—and other things—according to the Government Accountability Office (GAO).
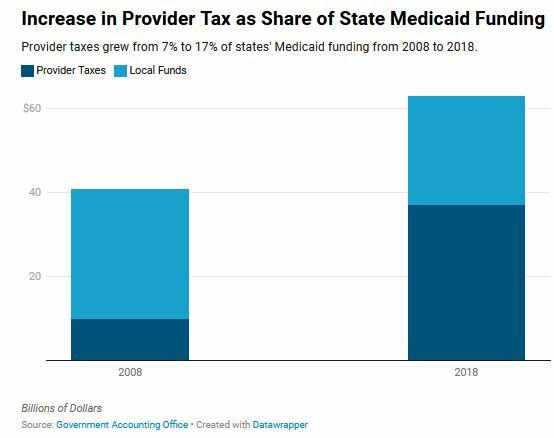
From 2008 to 2018, the share of states’ Medicaid spending covered by provider taxes grew from 7 percent to 17 percent according to the GAO.
In 2018, states received $63 billion in provider taxes and local government funds, according to GAO estimates. Of that amount, $16 billion (25 percent) was not used to pay providers.
That shifted 5 percent of the cost of Medicaid from the states to the federal government, the GAO estimates. The practice also resulted in lower overall reimbursement to some providers when accounting for their tax payments.
When measured as a percentage of the nation’s gross domestic product (GDP), a common measure of the country’s total wealth, the burden of providing Medicaid remained the same for states from 2008 to 2023. While overall spending went up, the economy was growing, too, so state Medicaid spending was essentially flat according to the think tank Paragon Health Institute.
Yet the overall cost of the program increased dramatically, meaning that the federal government paid the entire increase in the cost of the program over 15 years, according to Paragon.
Over that same period, the federal government’s share of the total cost of Medicaid grew from 60 to 72 percent.
Read the rest here…
Tyler Durden
Tue, 03/11/2025 – 12:05


